:format(webp)/cdn.vox-cdn.com/uploads/chorus_image/image/71542089/GettyImages_1388148275.0.png)
Years after it was first proven to work, a new tool for preventing sexually transmitted infections (STIs) is now closer than ever to entering mainstream medicine.
That tool is doxyPEP, an antibiotic that works like a morning-after pill — but instead of preventing pregnancy within hours of unprotected sex, it prevents STIs like chlamydia and syphilis. Ever since a 30-person trial first suggested hope for the strategy in 2015, people worldwide have begun trying doxyPEP for themselves, often without the approval or supervision of a medical provider.
Its use is gaining traction in the US. Last year, the San Francisco health department became the first authority in the US to recommend doxyPEP for men with recent STIs — especially syphilis — and for those who’ve had recent sex with men or trans women.
And its use is likely to expand. On October 2, the Centers for Disease Control and Prevention (CDC) published draft guidelines intended to educate health care providers on why, how, and when to prescribe doxyPEP to patients. (People can submit comments on the guidelines until November 16, and a final version will likely be published months down the road.) If they remain unchanged, the CDC’s guidelines could result in many more doxyPEP prescriptions for gay men, trans women, and those in their sexual networks — especially those at highest risk of getting infected with a bacterial STI.
Sexually transmitted infections have been rising in recent years, with syphilis in particular spreading explosively, and doxyPEP could help turn back the tide. Rising STI rates are costing dollars and lives: The CDC estimates that the US spent $1.1 billion on bacterial STIs in 2018, and 166 infants died in 2021 as a consequence of a syphilis epidemic affecting women of childbearing age.
Why did it take so long for the CDC to get behind doxyPEP? The major obstacle has been the fear that doing so would touch off a perilous game of infectious disease whack-a-mole — that in trying to mitigate one public health crisis, we’ll worsen another one.
Doxycycline, the medication in doxyPEP, is an antibiotic. Worldwide antibiotic resistance is a major problem — and doxyPEP runs the hypothetical risk of exacerbating it. Disease-causing bacteria can evolve resistance when exposed to certain antibiotics, becoming more dangerous.
Among the experts I spoke to last fall, shortly after San Francisco’s endorsement of doxyPEP, there was no consensus about how to balance the risks of antibiotic resistance with the risks of STI infections. Some said dwelling too much on the resistance risk would deny marginalized groups the preventive options they need.
“For some reason, with gay men’s sexual health, we are always placing these theoretical risks higher than what’s actually happening in the community,” said David Holland, an infectious disease doctor and public health expert at Emory University, during a talk at a medical conference in October 2022.
On the other hand, many experts were still cautious. “We just want to be very, very careful that before we start really ramping up the use of doxycycline, we are being thoughtful about the potential ramifications, and that we really are looking at the data to make sure to understand how to optimize use,” said Philip Chan, a Brown University infectious disease doctor who directs the largest sexual health clinic in Rhode Island, in an interview last fall.
DoxyPEP is making its way into the minds of providers and the hands of patients, even as debate continues about how to ensure it does more good than harm. Here’s why the drug isn’t the silver bullet it might seem to be, and why it’s nevertheless a source of hope for so many.
Clinical trials suggest doxyPEP would work to reduce STIs — although it’s only been proven in men who have sex with men
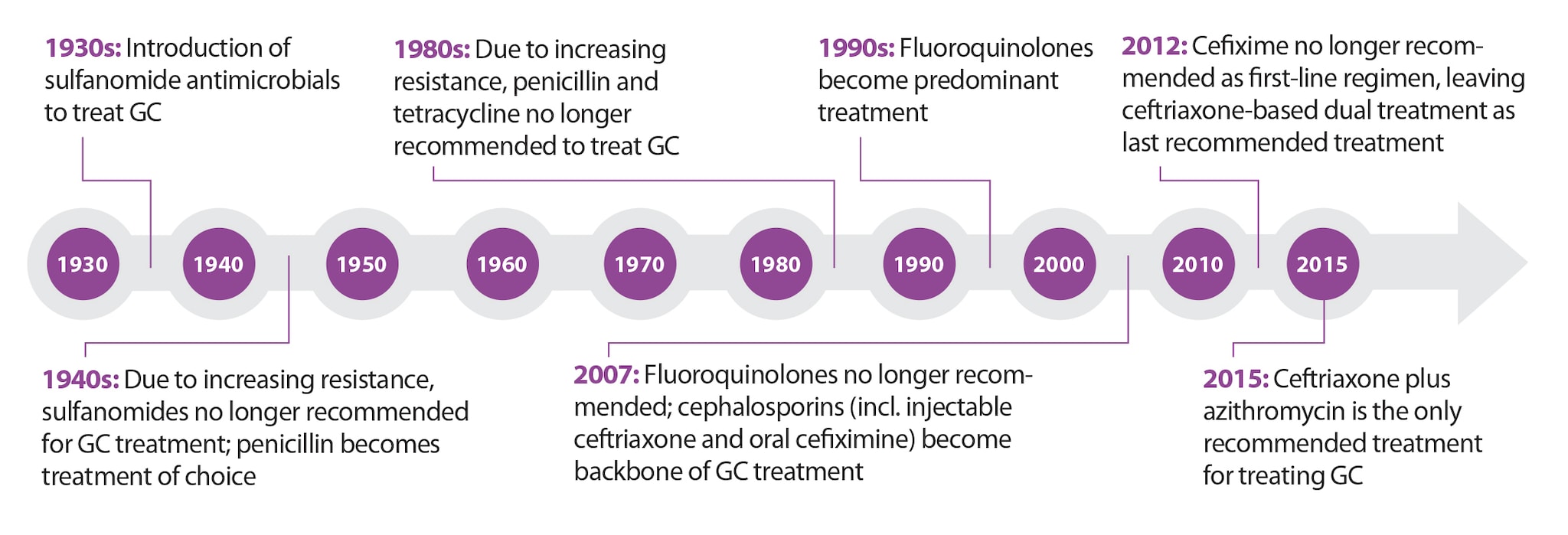
Doxycycline has plenty of street cred in the STI world. A week’s worth of the medication is the first-line treatment of choice for chlamydia, and a two-week course is the best syphilis treatment choice for people allergic to penicillin. (Doxycycline also sometimes works against gonorrhea, although the germ’s growing resistance to the medication means it is no longer recommended as a treatment for that infection.)
In contrast, doxycycline PEP is for preventing infection, not for treating it. “PEP” stands for post-exposure prophylaxis: The idea is that if a person takes a single dose of the medication soon enough after unprotected sex, any bacteria that might cause an STI would be killed before entrenching enough to cause a full-blown infection.
This “morning-after” approach to preventing STIs isn’t a brand new strategy: In the 1940s, the US Navy studied whether penicillin taken after sex prevented gonorrhea infection in men (it worked, at least for a time), and other trials studied the antibiotic minocycline for the same purpose in the 1970s. There’s also HIV PEP — distinct from PrEP — which has been incredibly effective at preventing infection after exposure to the virus by needlesticks (usually in health care settings) or during sex. HIV PEP contains antivirals that, like doxyPEP, help stop an infection before it has time to settle into the body.
The data to support doxycycline as PEP for STIs comes from two clinical trials in humans —one conducted in France, published in 2017, and one conducted in Seattle and San Francisco and published in April.
Both trials studied the drug’s use in men who have sex with men and trans women — populations who were chosen because they have the highest risk of infection, and therefore the highest likelihood of being helped by doxyPEP. The American trial studied the protective effects in both people with and without HIV infection, while the French trial included only people without HIV infection.
People who enrolled in the trials were randomly assigned to two groups: One group was given doxycycline pills and instructed to take two within 24 hours of unprotected sex, while the other group didn’t receive any drug. In both studies, everyone who participated was offered comprehensive services — education, condoms, and HIV PrEP counseling — aimed at reducing health risks during sex.
In both trials, doxyPEP was very effective in reducing bacterial STIs. The pill reduced infections by half in the French trial and by two-thirds in the American trial — such high efficacy that investigators stopped the trial early because it would have been unethical to continue not offering doxyPEP to people.
Notably, doxycycline didn’t have the same preventive oomph against all STIs. Protection against chlamydia and syphilis was strong in both studies, but in the trial conducted in France, doxyPEP offered little to no protection from gonorrhea infection. In the US, the results were better, with a 55 percent drop in gonorrhea cases among study participants taking doxyPEP.
The big difference in the US and French results is probably due to differences in gonorrhea’s resistance to doxycycline: While about half of all gonorrhea in France doesn’t respond to doxycycline, that proportion is closer to one-fifth in the US. (Notably, gonorrhea has been evolving resistance to antibiotics pretty much since antibiotics were developed — so its doxycycline resistance is really more indicative of gonorrhea’s resistance to a host of drugs than suggestive of a doxycycline problem specifically.)
A trial in Kenya to determine whether doxyPEP works as well in cisgender women as in the groups that have already been studied has yielded disappointing results: At a conference earlier this year, investigators presented data showing inconsistent effects on STI rates in women. (Notably, syphilis transmission in the study population was much lower than it is in American women.)
Although doxycycline isn’t a perfect preventive drug, it could help a lot, experts say. Even if it were only used in men who have sex with men and their sexual networks, doxyPEP would benefit everyone at risk for STIs, said Jeffrey Klausner, an infectious disease doctor at the University of Southern California specializing in sexually transmitted infections. That’s because it would reduce transmission among the people at highest risk for repeated infections, making onward transmission through other sexual networks less likely.
DoxyPEP would be a no-brainer — if it weren’t for antibiotic resistance
Even though doxycycline still has a few hoops to jump through before the CDC officially recommends it as STI prevention, sexual health providers can and do prescribe it that way. Doxycycline is a Food and Drug Administration-approved drug, and providers can prescribe it for uses beyond what it’s been approved for (known as “off label” prescribing).
As of last fall, about 10 percent of men who have sex with men in Europe and Australia were using the medication, often purchasing it from online pharmacies or sources that don’t require a prescription, and Facebook groups for HIV PrEP users teemed with testimonials and advice.
Plus, doxycycline is already used as a post-exposure pill — just not for STIs. The CDC recommends a single dose of the medication after a tick bite in areas with lots of Lyme disease, and one or more doses after exposure to water contaminated with the bacteria that causes leptospirosis, an infection that can lead to kidney and liver damage and even death.
If rising STI rates are such a public health emergency, why isn’t doxyPEP a slam-dunk?
One concern is doxycycline’s side effects. The drug causes digestive symptoms in anywhere between 4 percent and one-third of people who take it regularly, and has been linked to skin sensitivity in anywhere between 7 percent and one-fifth of people who take the medication. The American study looked for signs that drug-related discomfort was enough to stop people from using it, and found encouraging results: Not one of more than 500 study participants stopped taking the drug because of problems tolerating its side effects.
The much bigger worry is that doxyPEP could add fuel to another five-alarm public health fire: antibiotic resistance, which the World Health Organization has called one of the top 10 threats to global public health. Using antibiotics intermittently, or not taking enough of them when an infection is brewing, can be a recipe for producing so-called “superbugs,” germs that evolve to evade common antibiotics. The way this happens: If a group of germs doesn’t get completely saturated with an antibiotic, only the strongest ones — that is, those that would only be killed by much larger doses of the antibiotic — survive. Eventually, their offspring may be entirely resistant to that antibiotic.
(There’s no parallel risk with HIV PrEP because the antiviral medicine it involves doesn’t really have an effect on pathogens other than HIV. However, in the early days of HIV PrEP — since proven to be spectacularly effective at preventing HIV — health authorities were likewise hesitant to embrace it due to resistance fears that ended up being unfounded.)
The US-based trial is still evaluating the effect of doxycycline on antibiotic resistance in germs in the genital, respiratory, and digestive tracts of its 500-odd study participants.
When I spoke with her last fall, Annie Luetkemeyer, an infectious disease doctor and STI researcher at the University of California San Francisco who co-led the US study, said there isn’t any data suggesting that doxycycline is turning lots of microbial bad guys into broadly resistant supervillains. However, determining the drug’s potential to wreak resistance havoc isn’t as easy as just studying its effects on a few hundred individuals, said Chris Kenyon, an infectious disease doctor at the Institute of Tropical Medicine in Antwerp, Belgium, who specializes in antibiotic resistance among sexually transmitted pathogens, in a late-2022 interview.
If scientists really wanted to understand doxycycline’s resistance-creating potential, Kenyon said, they’d conduct huge studies that track people over several years — something like a study in a dozen cities, involving thousands of people. They’d look for patterns: Does more use of the drug lead to more signals of antibiotic resistance? Although studies like that exist for other antibiotics, we don’t have them for doxycycline, he said.
What we do have are studies of much smaller groups of people that show, on an individual level, that doxycycline can induce resistance among certain dangerous germs.
The drug has for decades been prescribed for people to use for months or even years at a time to prevent acne and malaria, and for maintaining chronic infections. A review of studies suggests that people who take long-term doxycycline brew a harder-to-treat version of Staphylococcus aureus, a potentially disease-causing bacteria in the nose.
That review also hinted that long-term doxycycline use leads people to develop resistant bacteria in the mouth and the gut. While some of these changes were reversible, none of the studies were designed to show what they meant in the long term, after those resistant germs had a chance to spread to others.
If doxycycline resistance were to occur and spread on a larger scale, it could render the medication less effective against important germs on a global level. Doxycycline is currently used to treat pneumonia and other infections everywhere, but especially in low-income countries — so removing it from the world’s antibiotic toolbox would be a big blow to global health.
The amount of doxycycline the world currently uses is a fraction of what it would end up using if doxyPEP is widely prescribed; in that case, doxycycline use would increase at least 800-fold over current consumption, according to Kenyon’s back-of-the-envelope calculations.
“It’s a massive exposure,” Kenyon said — and the chance that exposure would induce widespread resistance to doxycycline and other antibiotics is “staggeringly high.” But the data to prove that just doesn’t exist yet.
There is no perfect road ahead
This data vacuum lands differently for different experts. On one hand, said Kenyon, infectious disease doctors like him who see lots of untreatable infections may approach the strategy with more caution. “I would love it to be safe because I’m an STI physician,” he said. “But I don’t want to be telling my patients, ‘Look, this is a wonder medicine,’ until we’ve really nailed that. And I don’t think we’ll be in that place for years.”
But providers in the HIV PrEP world and the many people eager to take doxyPEP say its benefits can’t wait that long.
Sexually transmitted infections take an emotional toll on the communities where they take hold. Among men who have sex with men and their sexual networks, doxyPEP has some of the same potential that HIV PrEP did to restore a waning sense of agency, said Luetkemeyer.
“PrEP is exactly where we need to look for what this holds for us,” she said. Especially for people with HIV or taking PrEP, doxyPEP has people “finally feeling like they got a little bit of control and dignity in their lives,” she said.
“That’s a big thing.”
Update, October 13, 8:50 am ET: This story, originally published on October 25, 2022, has been updated to note the CDC’s new draft guidelines on doxyPEP.






{kind=link}
{kind=link}
{kind=link}